
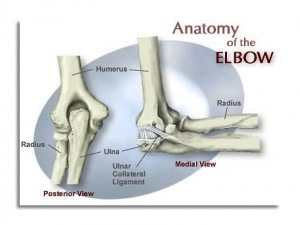
Predicting and Preventing UCL Injuries
Pitching coaches and researchers are pointing to mechanical flaws along with increased pitching velocities as the root cause of the large uptick in UCL tears. In the gym, we see a bunch of trends that have been correlated to UCL injuries either anecdotally or backed by research. The following are my top 3 red flags prior to a UCL injury from a thrower.
1. Cervical Rotation Dysfunction
Cervical rotation is depended on good joint mobility as well as enough flexibility from the muscles that attach to the neck and shoulder. What most people miss when evaluating or training rotational athletes is that core stability plays a huge role in cervical rotation.
The first video is of a left-handed pitcher supine with full right rotation in his neck.
The next video is of the same left-handed pitcher standing with limited right cervical rotation.
The inability to move properly through the neck while standing (especially in right cervical rotation) will lead to altered pitching mechanics. On the mound the result will often present as “flying open”. Pitchers with this type of dysfunction struggle with consistency of pitch location and velocity. They also tend to present with neck and shoulder pain prior to UCL damage.
One fix that we use with these athletes is half get-ups. Usually a few challenging with or without weight can correct this dysfunction long-term.
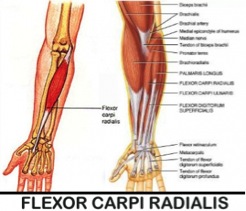
2. Tight Pitching Forearm
I have yet to find good literature on “forearm tightness” prior to UCL injury, but I can tell you from experience athletes who complain about forearm tightness on a regular basis that goes untreated often come back down the line with medial elbow pain, little leaguers elbow, or a UCL tear.
Studies have shown that the “flexor-pronator” muscles are used when throwing to create elbow stability.1 My suspicion is that where the body feels that it cannot control the violent valgus forces of the elbow during throwing, these forearm muscles (particularly the flexor carpi radialis) over-assist the passive restraints of the ulnar collateral ligament. This is a red flag that needs to be address immediately.
3. Lower Body Injury or “Balance Issues”
Fluid transfer of force from one joint to the next is the basis for great movement, injury prevention, and high performance. Ignoring foot, ankle, and knee injuries while jumping back into high level throwing is asking for trouble up the kinetic chain.
Garrison et. al compared baseball players who had no UCL tears vs. players who did. Each group completed the Y-Balance Test, a quantitate test to measure overall balance. Participants with a UCL tear demonstrated decreased performance for their stance and lead lower extremities during the Y-Balance Test. The researchers concluded that there is a potential link between impaired balance and UCL tears in high school and collegiate baseball players.
I put “balance” in quotations because I believe there is a wild miss understanding of what real balance issues are. True balance issues come from the vestibular system. Most of what we see with younger athletes is very poor strength and an inability to express strength or movement in a given range of motion. When someone says they have a balance issue when standing on one leg, I hand them 2 heavy dumbbells to hold next to their body and stand on one leg again. By holding the weight and crushing the dumbbells with their hands, they activate their hips and core musculature giving their body feedback to remain stable. If you try this little test and your single leg stance does not improve, you likely have some true underlying balance issues and should get that checked out. For the rest of you, you need to get stronger!
Move Better, Get Stronger, Prevent UCL Injuries
1. Park MC, Ahmad CS. Dynamic contributions of the flexor-pronator mass to elbow valgus stability. J Bone Jt Surg. 2004;86(10):2268-2274.


Leave a Reply