Mechanical Training With ATP Increased Throwing Velocity +7 MPH In Two Weeks
There are so many ways to address someone’s needs in a throwing program. Here is a case study of a remote programming client seeing good results with his training, but needing some tinkering with his throwing mechanics.
Kaito, highlighted here, is using 9oz balls to repattern his arm action and load. As you can see in the video, his hand goes from below his elbow at ffc to above and there are significant changes in his hip: shoulder separation.
As we progress, there are other mechanical changes we will address, but for the time being, we will continue to push Kaito’s new mechanical changes as well as lock in his velocity gains. His previous mound velo was 84mph, but with his recent changes in mechanics and fixing issues with his force-velocity curve, we know he mid-90s in the tank.
To schedule a mechanical consultation with Dr. Heenan via email: jheenan@advancedtherapyperformance.com
Shoulder Pain in Baseball Players
Anterior (front) shoulder pain is one of the most common complaints we get from all overhead athletes especially baseball players. This pain is often palpable at the origin of the bicep tendon. Although every case can have countless pathologies (such as labral tears, impingement, poor movement mechanics) causing the pain at the bicep tendon region, about 90% of the time we find that this pain is referred pain.
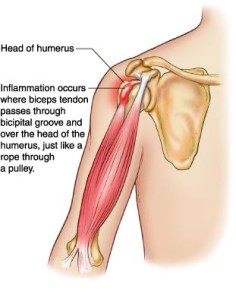
Referred pain is pain felt in a part of the body other than its actual source. Through my studies of Chinese Medicine, I can validate that many times the science and theory behind referred pain make little sense. Fortunately, pain that would be considered “bicipital tendonitis” is often very clear cut referred from the rotator cuff— most specifically the infraspinatus. The “X”s in the image below shows how the infraspinatus connects to the humerus (arm bone). Altered length, strength, movement mechanics, tissue quality or timing of the infraspinatus will throw off the mechanics of overhead movements.

To determine if this a true referred pain issue, we find the painful motion (usually reaching overhead) and have the athlete give us a number 1-10 (10 being terrible pain). After establishing a baseline for pain, we find tender points in the infraspinatus, apply firm pressure and retest the motion. This is uncomfortable for the athlete in the spot being pressed but often brings a 6-8/10 pain down to a 0-1. If that is the case, we have found the problem.
Fixing the soft tissue quality is usually done by aggressive treatment. This can be active release, cupping, Graston’s, or Gua Sha. Cupping has been the tool that gets the quickest and longest lasting results (see below). I believe this is the case because almost all therapeutic techniques are compressive in nature. Cupping offer a decompressive component often causing discoloration. Most athletes walk away pain-free in 1-2 treatments even if they have been suffering symptoms for years.
If you do not have access to a manual therapist, a lacrosse ball jammed into the infraspinatus often does the trick.
Move Fast, Throw Hard, Live Well – Development is a process, not a destination.
With the draft only a few days away, this list will bode well for many of my clients and readers hoping to one day be drafted.
88 percent of NFL draft picks played multiple sports

“According to TrackingFootball.com, 224 of the 256 players chosen during the draft were multi-sport athletes in high school. Of all draftees, 63% participated in track and field, 48% played basketball and 10% played baseball.”
Research has been pointing athletes towards playing multiple sports for maximum athleticism and decreased risk of overuse injury for years now. In my collegiate and clinical coaching experience, anecdotal evidence has been overwhelming that multi-sport athletes are healthier and reach high levels than their specialized counterparts.
Cubs manager Joe Maddon speaks out against specialization
“I hate the specialization with kids, when they’re playing on these travel squads when they’re like 12, 13, 14 years old, only dedicated to one thing, Traveling all the time. Paying exorbitant amounts of money to play baseball with hopes they’re going to become a professional baseball player. “I think that’s crazy. I love cross-pollination when it comes to athletes, You get guys that did not just play baseball, meaning they’ve been around a different set of coaches and styles and ways to get in shape and thoughts. I love that.” Maddon said
Many parents I speak to are terrified that their child will not be prepared to play a high level of high school sport, will not get a scholarship, and will not get drafted. I understand the worry, but many are racing the wrong race. The goal should be to maximize enjoyment of the game, become as athletic as one can become, and keep on developing. Development is a process, not a destination.
3 Eating Secrets to Bulk Up Fast

This week I have been bombarded with muscle gain and weight gain questions. With the summer approaching, many athletes are looking to pack on weight while playing and training hard. This can be tough, but is done every year in our gym— usually 20-30lbs in a 3-month window. These three tips help many of our ball players stay on track during these bulking phases.
Predicting and Preventing UCL Injuries
Pitching coaches and researchers are pointing to mechanical flaws along with increased pitching velocities as the root cause of the large uptick in UCL tears. In the gym, we see a bunch of trends that have been correlated to UCL injuries either anecdotally or backed by research. The following are my top 3 red flags prior to a UCL injury from a thrower.
1. Cervical Rotation Dysfunction
Cervical rotation is depended on good joint mobility as well as enough flexibility from the muscles that attach to the neck and shoulder. What most people miss when evaluating or training rotational athletes is that core stability plays a huge role in cervical rotation.
The first video is of a left-handed pitcher supine with full right rotation in his neck.
The next video is of the same left-handed pitcher standing with limited right cervical rotation.
The inability to move properly through the neck while standing (especially in right cervical rotation) will lead to altered pitching mechanics. On the mound the result will often present as “flying open”. Pitchers with this type of dysfunction struggle with consistency of pitch location and velocity. They also tend to present with neck and shoulder pain prior to UCL damage.
One fix that we use with these athletes is half get-ups. Usually a few challenging with or without weight can correct this dysfunction long-term.
2. Tight Pitching Forearm
I have yet to find good literature on “forearm tightness” prior to UCL injury, but I can tell you from experience athletes who complain about forearm tightness on a regular basis that goes untreated often come back down the line with medial elbow pain, little leaguers elbow, or a UCL tear.
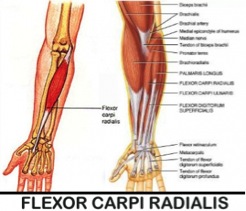
Studies have shown that the “flexor-pronator” muscles are used when throwing to create elbow stability.1 My suspicion is that where the body feels that it cannot control the violent valgus forces of the elbow during throwing, these forearm muscles (particularly the flexor carpi radialis) over-assist the passive restraints of the ulnar collateral ligament. This is a red flag that needs to be address immediately.
3. Lower Body Injury or “Balance Issues”
Fluid transfer of force from one joint to the next is the basis for great movement, injury prevention, and high performance. Ignoring foot, ankle, and knee injuries while jumping back into high level throwing is asking for trouble up the kinetic chain.
Garrison et. al compared baseball players who had no UCL tears vs. players who did. Each group completed the Y-Balance Test, a quantitate test to measure overall balance. Participants with a UCL tear demonstrated decreased performance for their stance and lead lower extremities during the Y-Balance Test. The researchers concluded that there is a potential link between impaired balance and UCL tears in high school and collegiate baseball players.
I put “balance” in quotations because I believe there is a wild miss understanding of what real balance issues are. True balance issues come from the vestibular system. Most of what we see with younger athletes is very poor strength and an inability to express strength or movement in a given range of motion. When someone says they have a balance issue when standing on one leg, I hand them 2 heavy dumbbells to hold next to their body and stand on one leg again. By holding the weight and crushing the dumbbells with their hands, they activate their hips and core musculature giving their body feedback to remain stable. If you try this little test and your single leg stance does not improve, you likely have some true underlying balance issues and should get that checked out. For the rest of you, you need to get stronger!
Move Better, Get Stronger, Prevent UCL Injuries
1. Park MC, Ahmad CS. Dynamic contributions of the flexor-pronator mass to elbow valgus stability. J Bone Jt Surg. 2004;86(10):2268-2274.
Move Fast, Throw Hard, Live Well – If You Are In Pain Get Treated ASAP- Direct Access
Today’s post is going to be quick as I am off to talk to the Fairfield American Little League Program’s coaches about injury reduction and red flags with their athletes.
One of the main points I try to make at these talks is to refer out ASAP if there is pain. Orthopedic doctors are great, but in most cases it’s more advantageous to see a qualified Physical Therapist or Chiropractor first.

Back Pain
Much of the research references acute lower back pain. Within the studies they show the typical cycle of back pain, waiting a few days, calling the orthopedists, waiting a few days to get an appointment, going to the appointment, getting an MRI and/or x-ray, then being referred to PT. In most states, Direct Access is available to walk directly into a Physical Therapy office and get treated. Some argue there is a fear factor, as PTs don’t do X-rays or MRIs, which I completely understand. In rebuttal to those claims, a good PT or Chiro will evaluate pain and immediately refer out if they believe you need a second opinion or diagnostic imaging.
“A 4 year study of Blue Cross Blue Shield of Maryland claims data and found that total paid claims for physician referral episodes to physical therapists were 2.2 times higher than the paid claims for direct access episodes. In addition, physician referral episodes were 65% longer in duration than direct access episodes and generated 67% more physical therapy claims and 60% more office visits. The HSR study looked at a far more extensive number of episodes than the previous study, and also controlled for illness severity and other factors that could have affected the patients’ outcomes.”1,2
60% more visits and cost is a large time frame and price to pay just for going to the Orthopedists!
The take home point of this info is not that going to the doctor is a bad thing, but waiting around for your pain- regardless if its back, elbow, neck, knee, hip, whatever- to subside magically instead of getting treatment will cost you in the long run; both in time and money. Have a trusted team of professionals to turn to immediately when you are in pain, and if you need the opinion of your doctor those professionals will gladly send you their way, but wasting time to get into the doctor or for the pain to go away is just that, a waste.

Trusted Side Kick #1

Trusted Side Kick #2
Good luck to everyone in their seasons!
Works Cited
1. Pendergast J, Kliethermes SA, Freburger JK, Duffy PA. A Comparison of Health Care Use for Physician-Referred and Self-Referred Episodes of Outpatient Physical Therapy. Health Serv Res. 2012;47(2):633–654. doi:10.1111/j.1475-6773.2011.01324.x.
2. Mitchell JM, de Lissovoy G. A Comparison of Resource Use and Cost in Direct Access Versus Physician Referral Episodes of Physical Therapy. Phys Ther. 1997;77(1):10–18.
Move Fast, Throw Hard, Live Well- Little League Curveballs and Youth Weight Training
This weeks post I am going to share a readers question and my response about weight training his younger athlete. If you have a question you would like answered feel free to shoot me an email.
Enjoy!
Q:
What would you recommend for a 13 yr old 7th grader, honestly? I am not wanting him to do more than hi-rep, bodyweight exercises at most. He’s 5’9” (and growing), 110 lbs. throws pretty hard – has a nice arm, and I want to keep that intact. Staring the travel ball with a good, established organization in IL this year…what are your thoughts on throwing curve balls, if taught by a former pro pitcher, etc? (I am leery of that).
A:
As I said in the webinar, if you can play organized sports, you can train (and its safer!). High rep stuff is fine, but that’s where we usually see injuries because of fatigue and poor form. Moderate weights would be a better option for him. Move well and then move higher weights.
Here is my take on youth curveballs; research wise if it’s being taught properly (mechanically efficient) there is not a huge chance of injury. That being said, there are a ton of bad coaches out there (not that his is bad–I have no idea), but being a former pro doesn’t automatically qualify you to be a “good” or well researched coach.
From what I have seen in the rehab and coaching world, poor progression of throwing (jumping up in intensity or mainly volume) too quickly leads to lots of issues. The kids who throw “too many curveballs” are usually the kids who cant compete with just a fastball. And as I have written about before, skipping on fall/winter baseball is a must.
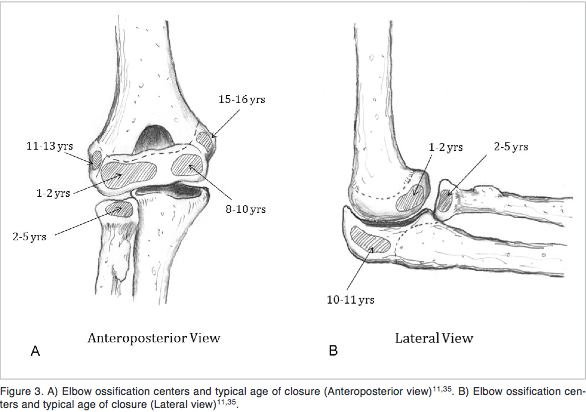
At this point in my career, if my child was a pitcher in little league I would encourage fastball and change up location and speed, that alone will keep batters off balance. Once they start shooting through puberty (13-15 years), I would let them play with curveballs with a coach that is highly qualified. I grew up with a coach who said “never two curves in a row” for both practice and play. Great rules to help set-up hitters and stave away from overuse.
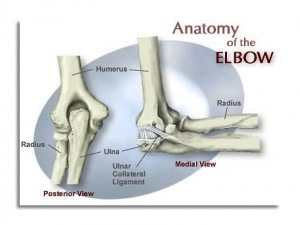
The image attached is a visual of when portions of the arm ossify. The medial epicondyle is the last to fully fuse and we should always proceed with caution.
On the other hand, Phil Rosengren does a great job at expressing why he thinks kids should be tough the curveball at a younger age. To be frank, I don’t disagree with any of his points. And to Phil’s credit, every athlete he has sent me has never had an elbow pathology.
Many people are racing for their kids to be on ESPN in the LLWS. I think they are racing the wrong race. I’ve had the opportunity to work with many kids whom have been on ESPN before the age of 13… some of what they are dealing with mentally are so unfathomable it’s disgusting. Not to mention some of the injuries I’ve seen especially from the “best” players on those teams.
Move Fast, Throw Hard, Live Well – Tommy John Surgery, Lactic Acid, and the Physiological Response to Pitching
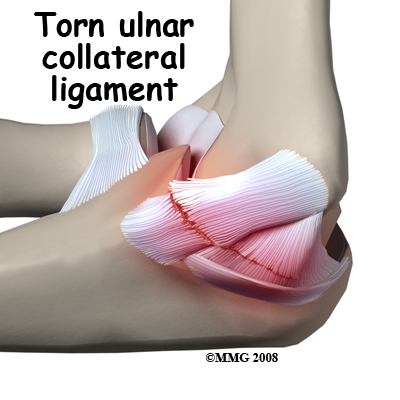
Mike Reinold, former Physical Therapist for the Boston Red Sox does an outstanding job at laying down realistic expectations in regards to ulnar collateral ligament (UCL) reconstruction. This is a must read for all pitchers!
The physiological responses to a single game of baseball pitching
This is an older journal article that takes an in-depth look at how the body responds to pitching 7 innings. The researchers provide intermittent data within the game and 24 hours post game.
It’s Not About the Lactic Acid: Why You’re Still Sore After Yesterday’s Ride (Workout)
Dr. Burke does a nice job at explaining the reasons why “lactic acid” is not the issue the day after a workout. I can’t begin to explain how often athletes, coaches, and parents talk about how they need to “clear the lactic acid” from the previous days workout. As Burke states “lactic acid is completely washed out of the muscles within 30 to 60 minutes after you finish riding. Since muscle soreness does not show up until 24 to 36 hours later, scientists have been exercising their brains to come up with another explanation.”
The next time a coach or trainer tells you are doing distance running as a “flush run” or “to clear lactic acid” start asking why, because the science in no way backs this claim.
Hip Arthroscopic and Incidences of Total Hip Replacement
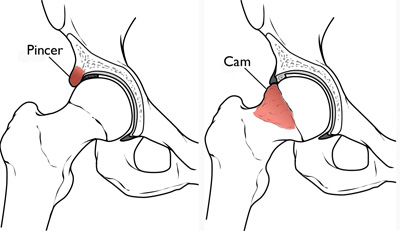
Earlier today I had a video consult with a 28 year old powerlifter with femoroacetabular impingement copmaining of hip pain while squatting, and atrophy of the glute medius region. This athlete had consulted with numerous surgeons and rehab specialists trying to figure out how to address his impingement with and without surgery. As the athlete noted, some surgeons he spoke with had a good grasp of what his options were and possible outcomes, while some had no idea and offered completely outdated information.
I sent him the following literature to highlight some of the more current research on possibly dodging a total hip replacement. As stated, there are no guarantees and every case is different, but some of the facts are very much in his favor.
“Attached is research on patients whom have an arthritic hip and had arthroscopic surgery. The study tracks incidents of total hip arthroplasty post-arthroscopic debridement. Out of 564 patients in the sample, only 16% (90 patients) eventually required THA over the 7-year period. The mean age for the subjects was 55 years old.
To me, this gives high hopes for a younger athlete like yourself whom wants to avoid having total hip replacement and wishes to compete at a high level. I think the most enlightening information from this study was “75% of the patients with severe OA did not require THA by the end of the study.”1
Obviously there are lots of variables for each patient, but with a great surgeon and rehab specialist you should mitigate a ton of your long term risks.”
The incidence of total hip arthroplasty after hip arthroscopy in osteoarthritic patients
1. Haviv B, O’Donnell J. The incidence of total hip arthroplasty after hip arthroscopy in osteoarthritic patients. Sports Med Arthrosc Rehabil Ther Technol SMARTT. 2010;2:18. doi:10.1186/1758-2555-2-18.